As I have explained before, I’m not a vaccine opponent — I’m a vaccine mandate opponent.
But we live in a democracy, and for nearly two years the rights and freedoms that were our birthright in purportedly free nations have been surrendered to the whims and models of public health officials who have been granted power without accountability.
Without direct accountability for their (many) failures, there cannot be trust. When repeated failure doesn’t result in termination and replacement, and we are instead held hostage to these incompetency repeat offenders by our elected governments – there should not be trust.
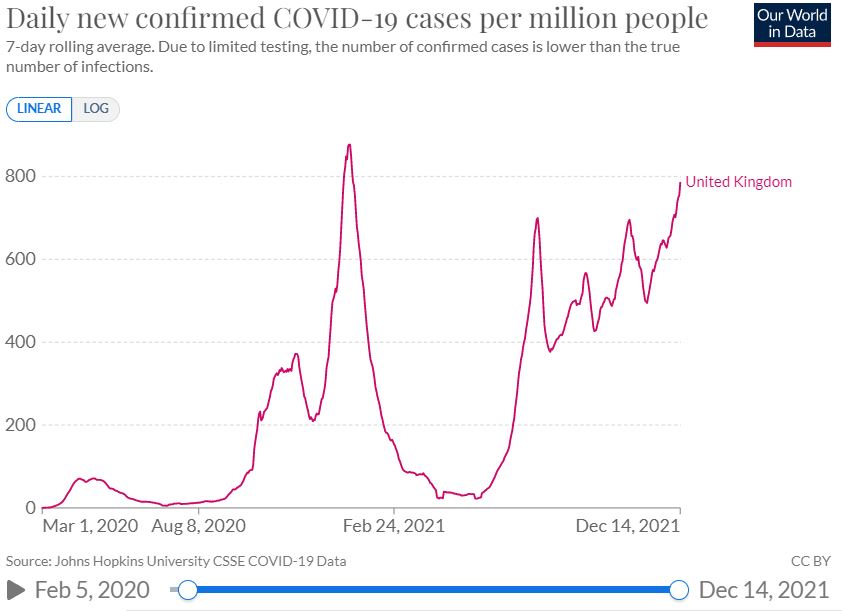
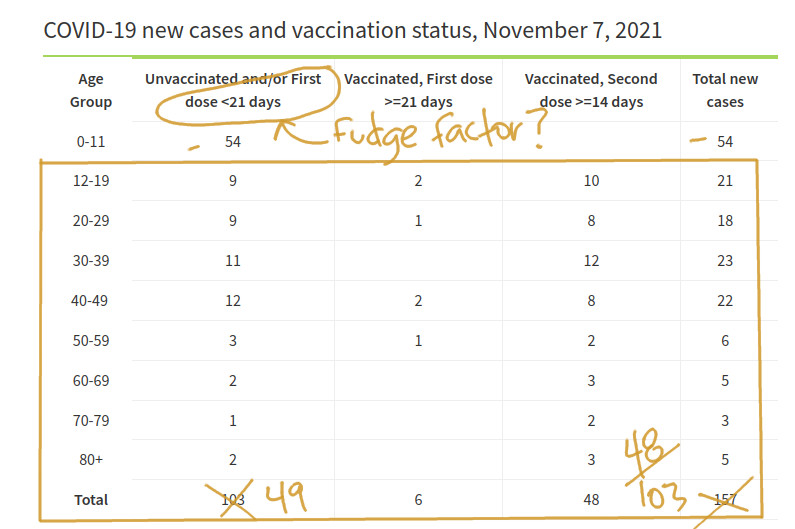
The Daily Sceptic has for some time been reporting on the apparent negative vaccine effectiveness visible in raw U.K. health data. Despite some age ranges now showing that the vaccinated are more than twice as likely to get Covid as the unvaccinated, this is routinely adjusted out, leading UKHSA to un-intuitively claim that the vaccines are still highly effective even against symptomatic disease.
A recent post by new contributor Amaneunsis explains the Test Negative Case Control approach (TNCC) used by authorities and researchers to adjust the data, and demonstrates that while a theoretically powerful way to remove some possible confounders, it rests on an initially reasonable-sounding assumption that vaccines don’t make your susceptibility to infection worse:
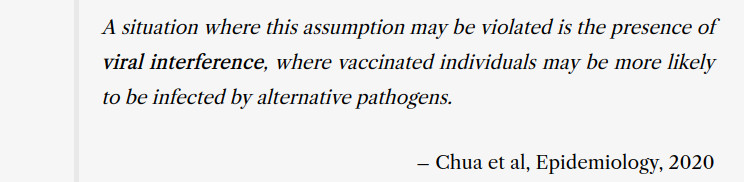
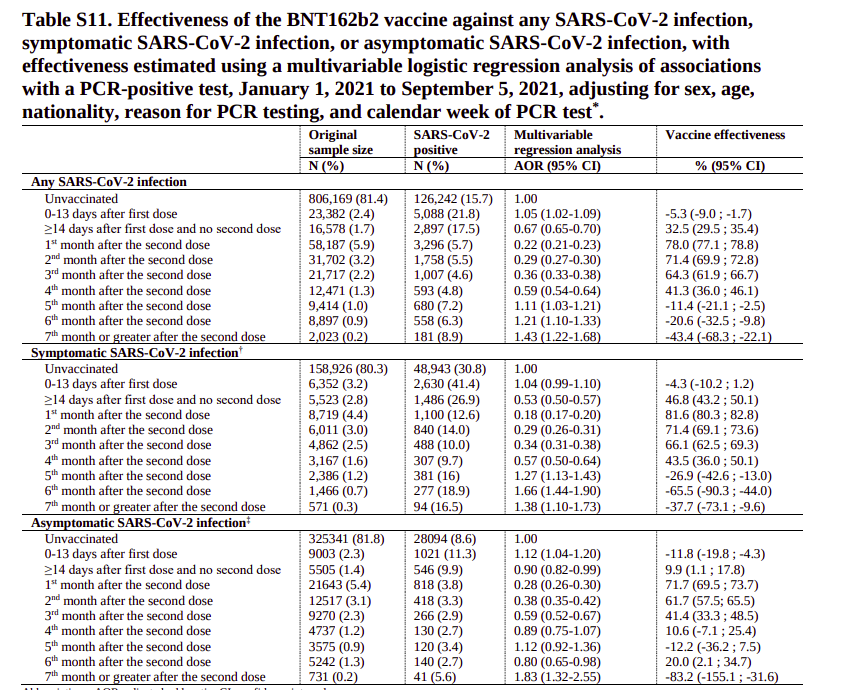
Amanuensis then compares results between the two different statistical approaches in a Qatari study to explore whether violation of this assumption is a realistic possibility and concludes that the multi-variate logistic regression found in their appendix supports the idea that viral interference can start happening a few months after initial vaccination.
What other angles can we explore this idea through? One way is to read the literature on prior epidemics.
H1N1
Between 2009-2010 there was a pandemic of H1N1 influenza, better known as Swine Flu. In April 2009 a small outbreak was detected in northern British Columbia. Researchers from Canada’s public health agencies researched the outbreak by doing interviews, testing and sero-surveys of the affected population. They were especially interested in the question of how effectively the routine trivalent influenza vaccine (TIV) was protecting people against H1N1.
The effect they saw was unexpected and previously unknown: people who had taken the flu vaccine had a more than doubled chance of getting sick with flu during the H1N1 outbreak […]
This result was shocking to the researchers. They were well aware of the impact these results could have on public support for the influenza vaccine programme and thus they didn’t merely double check their results, or request another team replicate their findings. They waited a year and a half, until six different investigations were all saying the same thing.
Emphasis mine.
So long as the voiced concerns of front line doctors are sanctioned and silenced, and legitimate inquiry about this vaccine’s efficacy and safety profile is countered with defamation and threats, instead of transparency and debate — those discussions will be hosted here.
The fact that papers published as recently as 2018 are talking about negative vaccine effectiveness as a new, not really understood effect should give governments serious pause for thought. Most people in public health are clearly unfamiliar with this phenomenon – as indeed we all are – and are thus tempted to either ignore it, delete it from their data, or try to convince the public that it must be a statistical artefact and anyone talking about it is guilty of spreading “misinformation”. The reports in these papers provide recent evidence that vaccines making epidemics worse is in fact a real phenomenon and that it has been previously detected by serious researchers who took every effort to avoid that conclusion.
Read it all, (and the reference links, too) as we always should.
Related: FDA is asking for 55 years to release the data they used to approve the Pfizer vaccine.