
People are pushing the panic button.
As of Sunday, the province has the highest rate per capita of COVID-19 infections in all of Canada, at a seven-day average rate of 33.1 cases per 100,000.
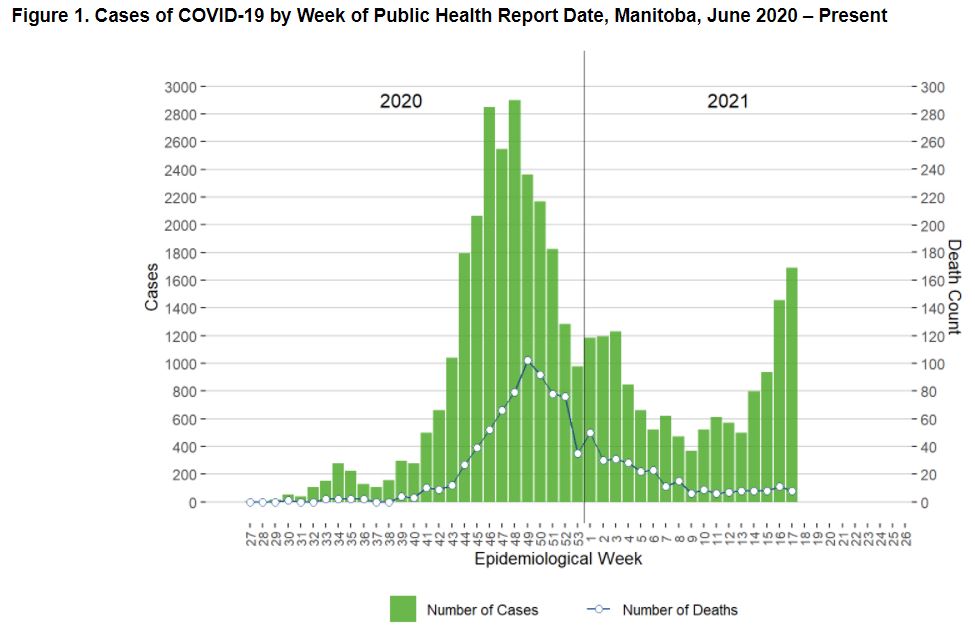
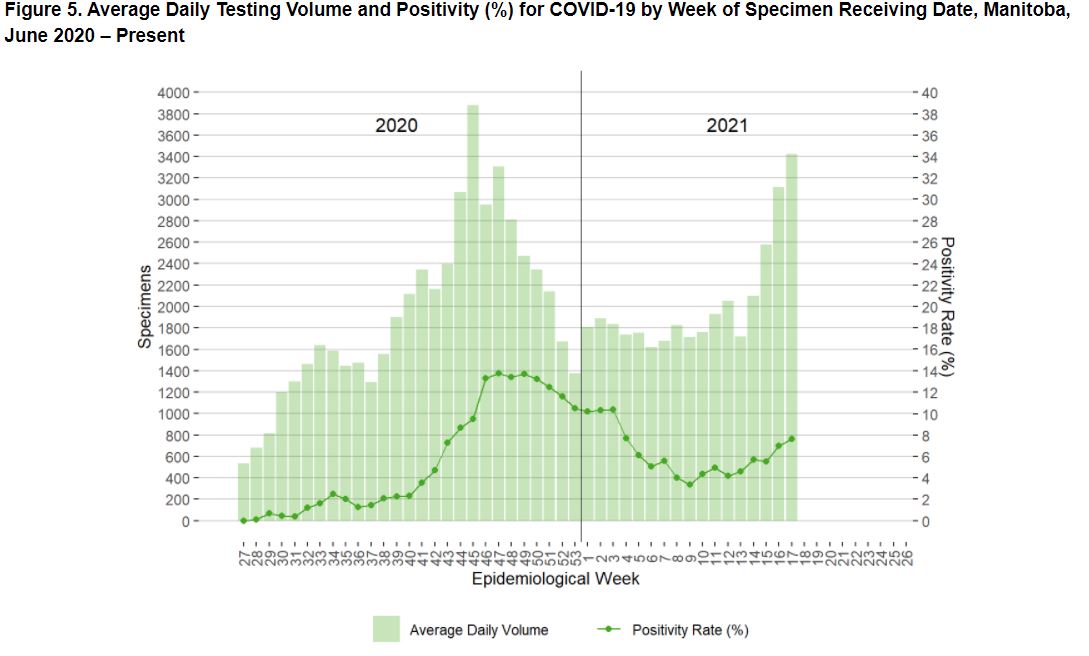
It’s not nothing. Hospitalizations are up and there’s a record number of covid patients in the ICU’s. But there is some context not being mentioned, death’s are way down, testing is also at an all time high, but the test positivity rate is well below what we saw in November and December. As we can see from the charts. (Click on charts to enlarge.)
And how many of these “cases” and hospitalizations were already vaccinated?
According to Dan Lett’s propaganda piece in Saturday’s Free Press, all Manitoba needs to do is be like New Zealand. Then everything will be peachy keen. Not sure why he doesn’t recommend fencing off the whole province, since that’s the only way for us to become a literal island. Maybe he’s worried about sounding too much like Trump.
According to what I read from Ontario recently, about .06% of the Covid cases are of people who have received one dose. So if it’s that effective, why can’t at least one-dosers be allowed to return to normalcy?
See: ‘Victory Lap’ below. Gerragos enumerates the correlations of lockdowns to HUGE spikes in COVID transmission. Seems the “scientific” advice was horribly WRONG … and deadly. But science is inerrant … right? Therefore the spikes weren’t caused by shutting people up in small enclosed spaces … but it must be that people were negligent in not wearing their masks. Sheesh.
The lockdowns DO cause the disease to spread more rapidly there’s no question. Where does this disease spread the most? INDOORS. What do lockdowns do? Force families to stay indoors with each other and get each other sick. Look at Surrey BC for a perfect example. They have a huge indocanadian population and it’s pretty common for them to have multiple generations in the same household. Wouldn’t you know it, Surrey BC is the capital of BC in terms of covid.
The panic button is all they have left….
slaw,
“The panic button is all they have left….” Um, didn’t Hilary give it to the Russians a few years back? Or, maybe it was the great reset button. Either way, Russia seems to have a bunch of the West’s buttons, and based on our current idiotic predicaments, maybe we should ask them to give the buttons back, cuz we need em!
I guess we could just ask Staples to make some more.
Before anyone criticizes this sarcastic post, they should consider how far we’ve already gone down the rabbit hole, and maybe, just maybe, this sarcasm is more realistic than the predicaments we’re all wallowing in, thanks to our “wise” leaders. These miscreants are not our friends, and until we accept this as the answer that has any semblance of truth and reality in our topsy turvey world, we’ll not be able to survive the future they are planning for us all.
We are getting close to ICU capacity, that is the concern. If that number was lower the health orders would be different. Manitoba is only averaging 12k vaccine doses per day. Should be able to do 25k+. But it is consistent, we are at over 60% of all adults receiving one dose.
In other news I got my JJ shot at the Drayton ND rest area. Thank you Pallister, governor Burgum and even you Former President Trump!
I have lived in Manitoba since 1978. Every single year without fail there has been panic about hitting ICU capacity due to flu. So this year it’s COVID not flu. Big whoopee. The real question is why is our ICU capacity so pathetic???
I think it’s the same in every province across the country. There is a shortage of ICUs because almost every gov’t cut back on health care.
I don’t think our politicians recognize the impact of the rising population on the health care system even though many of them want to increase immigration numbers while decreasing health care spending.
It seems like health care is an “easy” cut and I’m not smart enough to figure out a solution. Oh, wait…increase taxes…said no politician EVER.
The propaganda is changing from ‘you die’ to you will have consequences for the rest of your life.
“6-monts consequences of Wuhan virus in patients discharged from hospitals: a cohort study.” (my edit for clarity)
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)32656-8/fulltext
This place has done some analysis of post mortem as it were and concluded that the people who had the Wuhan flu are basically back to being neurotic, sick of it, can’t sleep well and so on and so on.
Seems they are back to normal.
I had it and it was a nothing-burger. Tightness in my upper chest and a very mild dry cough. If I didn’t know about the Dread Covid, I’d have assumed it was a weak-ass cold.
Good for you, however silly that may sound, though it would then follow that you are safer than those that got vaxed.
Unfortunately I had to do it to see my grandchildren.
Thanks for telling of your experience.
There is lack of that.
Lev, it sucks you were “forced” to get the vaccine. I can see that happening with me and my wife because we want to do some traveling after we retire. I REALLY resent it.
If the clowns in the Manitoba Health system would crank down the cycles of the PCR test to where the CDC says they should, the Covid would likely go away as they likely have many false positives. CDC guidelines say 28 cycles should be the max for the PCR test. Manitoba is running the test at 40-45 cycles. At that rate, they could prove an avocado has Covid.
Its not the positives that are the problem. Its the people in ICU.
Show me the numbers of those in the ICU who wouldn’t be there due to some other health issues anyway and I might get concerned.
What a a ridiculous statement.
Almost every Canadian hospital runs at close to maximum capacity in the ICU. When my late wife had a stroke in 2015, the ICU at the hospital was full. I walked through it every day for 5 days and it looked like EVERY bed was occupied.
Besides, the Ontario gov’t has had more than a year to take action on this issue and they failed. They built a few field hospitals to deal with the overflow and from what I understand, most of them have been dismantled.
Short staffed?
Not being used?
I don’t know what the answer is but I can say the Ford gov’t fuc&ed things up. He listened to the wrong “advisors” and cost the province dearly.
oh no, lets run and hide. Show me dead people and then you can run and hide. same shit, all lies, day after day. have I mentioned that Canadians ARE VERY F-ING STUPID?
India OK’s ivermectin and hydroxychloroquine for use to treat Covid, cases are plummeting and the CCP, WHO, Fauci, Gates and Soros are pissed. Big pharma is pissed.
Good on India giving the fuckers a stiff middle finger!
Manitoba has over 40% of its budget in the form of Transfer Payments from Justin Castro so they’ll do whatever it takes to land lots of federal money. Hair on fire panics are great as long as there is moolah attached to it. Saskatchewan, on the other hand, isn’t dependent upon Transfer Payments to the same extent as Manitoba and well, you do the math.
https://www.jccf.ca/manitoba-chief-microbiologist-and-laboratory-specialist-56-of-positive-cases-are-not-infectious/
Oops.
“The Justice Centre’s expert medical witnesses, Dr. Jay Bhattacharya, world-famous epidemiologist and Professor of Medicine from Stanford University, and Dr. Thomas Warren, infectious disease specialist and medical microbiologist, both provided evidence that the PCR test is unreliable in determining whether a person is infectious with the actual Covid-19 disease.
Chief Microbiologist and Laboratory Specialist Dr. Jared Bullard is a witness for the Manitoba government in this hearing. Questioned under oath by Justice Centre lawyers on Monday May 10, Dr. Bullard acknowledged that the PCR test has significant limitations. The head of Cadham Provincial Laboratory in Winnipeg, Dr. Bullard admitted that PCR test results do not verify infectiousness, and were never intended to be used to diagnose respiratory illnesses.
Dr. Bullard testified that PCR tests can be positive for up to 100 days after an exposure to the virus, and that PCR tests do nothing more than confirm the presence of fragments of viral RNA of the target SARS CO-V2 virus in someone’s nose. He testified that, while a person with Covid-19 is infectious for a one-to-two week period, non-viable (harmless) viral SARS CO-V2 fragments remain in the nose, and can be detected by a PCR test for up to 100 days after exposure.
Dr. Bullard testified that the most accurate way to determine whether someone is actually infectious with Covid is to attempt to grow a cell culture in the lab from a patient sample. If a cell culture will not grow the virus in the lab, a patient is likely not infectious. A study from Dr. Bullard and his colleagues found that only 44% of positive PCR test results would actually grow in the lab.
Dr. Bullard’s findings call into question the practice used in Manitoba (and elsewhere in Canada) of the results of classifying positive PCR tests as “cases,” which implies infectivity. Equating positive PCR tests to infectious cases, as so many provinces have done over the course of the past 13 months, is incorrect and inaccurate, according to this Manitoba Government witness.
Dr. Bullard acknowledged that he has been closely studying the correlation between Cycle threshold (Ct) value and infectiousness since at least May 7, 2020. Dr. Bullard acknowledged that Manitoba has known for some time that a given PCR test’s Ct value is inversely correlated with infectiousness. This means that testing for Covid at higher threshold levels can result in false positives as explained in this article. Even the World Health Organization (WHO) notes that careful interpretation of weak positive results is needed.
Weak results are those run at higher thresholds (more cycles). For example, someone with a positive PCR test that is run at 18 cycles is more likely to be sick and infectious than someone who has a test run at a Ct value of 40.
Dr. Bullard confirmed this was one of the first studies of its kind linking Ct value to infectiousness, and his study confirmed the findings of other studies in France and elsewhere.
Dr. Bullard also testified that Ct value (how many amplification cycles were used in a given PCR test to reach a positive test result) is significant as a proxy or indicator for infectiousness.
However, despite Dr. Bullard’s findings and recommendations in his two peer-reviewed studies, Manitoba still does not consider Ct values as a proxy for infectiousness in its public health response to Covid-19. Both Dr. Bullard and Manitoba Chief Medical Officer Dr. Brent Roussin confirmed under cross-examination that Ct values are not provided to public health officials by laboratories. Dr. Roussin admitted that he could mandate that the Ct value be provided to him, but that he has not done so.
Some jurisdictions, for example Florida, do consider Ct value in their public health response to Covid.
Finally, it should be noted that some Canadian news agencies have quoted Dr. Bullard as testifying that a positive PCR tests indicates infectivity 99.9% of the time. This is incorrect. Rather, Dr. Bullard testified that a PCR test will detect any viral RNA that is present in a sample 99.9% of the time. However, Dr. Bullard testified that determining whether or not a sample is actually infectious (containing a viable virus, capable of replicating) needs to be confirmed by lab culture. As noted, only 44% of the “positive” samples using a Ct of 18 returned a viable lab culture. Samples tested at a Ct of over 25, according to Dr. Bullard’s report, produced no viable lab cultures.
Manitoba has confirmed that it utilizes Ct’s of up to 40, and even 45 in some cases. This indicates “cases” resulting from such tests (above a Ct of 25) are almost certainly not actually infectious.
The hearing into Manitoba’s response to Covid and its violation of Charter rights and freedoms continues this week.”